If someone at your gym finds out you’re on TRT, there’s a decent chance they’ll give you a look. The one that says: yeah, sure, “therapy”. Because in a lot of gym circles, TRT and steroids get lumped together as the same thing with different excuses attached. They are not the same thing. Not physiologically, not legally, not in terms of what they do to your body, and not in terms of intent.
This article breaks down the actual difference. Not to defend anyone’s choices, but because the conflation of the two is genuinely misleading, and understanding what each actually is changes the conversation entirely.
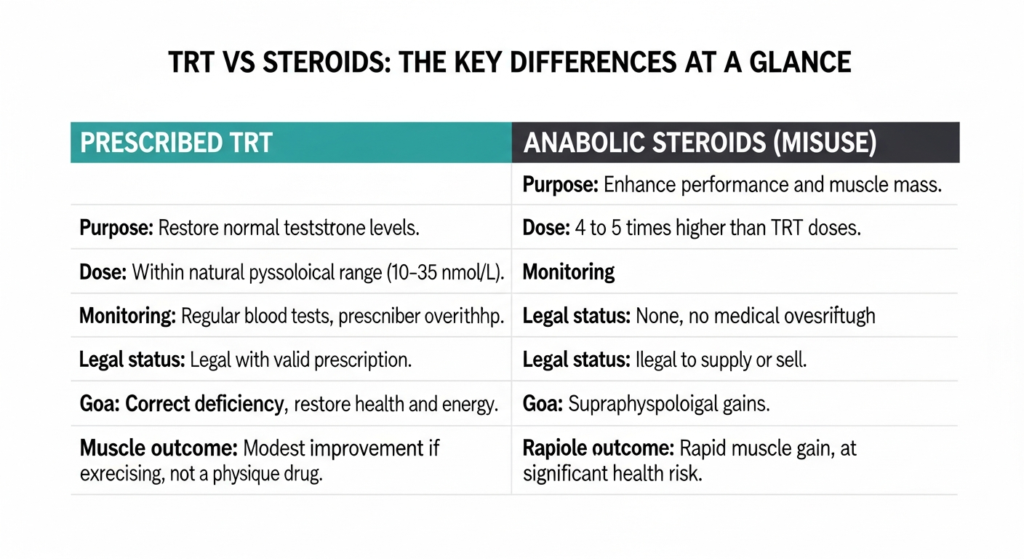
TRT and anabolic steroid use differ in purpose, dose, monitoring, legal status, and physiological outcome. The confusion between the two comes from the fact that both involve testosterone, but that is roughly where the similarity ends.
Let’s start with the technical truth
Testosterone is technically a steroid hormone. All steroid hormones are made from cholesterol and share a similar molecular structure. In that purely biochemical sense, yes, testosterone is a steroid. So are cortisol, oestrogen, and progesterone. The word “steroid” in chemistry describes a molecular structure, not a category of gym drugs.
When people say “steroids” in a gym context, they mean anabolic-androgenic steroids (AAS) used to enhance performance and muscle mass, often at doses far exceeding anything the body produces naturally. When doctors say TRT, they mean testosterone replacement therapy: a medically prescribed treatment to restore testosterone levels that have fallen below the normal range.
The clinical distinction is explained clearly on Voy’s breakdown of whether testosterone is a steroid, and it is the most straightforward summary of the actual difference I’ve found. The short version: TRT uses the same molecule, but the dose, the intent, the monitoring, and the physiological outcome are categorically different.
The dose is where the real difference lives
This is the most important thing to understand. The difference between TRT and steroid use is not primarily a legal or ethical one. It is a pharmacological one. Dose is everything.
Normal male testosterone levels range from roughly 10 to 35 nmol/L. TRT aims to bring levels that have fallen below this range back into it. The doses used are calibrated to restore physiological levels, not exceed them. The goal is to get your testosterone to where it would be if your body was producing it normally.
Anabolic steroid use for performance enhancement involves doses that push testosterone levels four to five times higher than TRT doses, and significantly above the natural range. Research (Bhasin et al., 1996, NEJM) showed that supraphysiological testosterone doses, in the range of 600mg weekly versus a physiological replacement dose of around 100 to 150mg weekly, produced significant muscle gains. But the doses required to get those gains are in an entirely different category from what any clinician would prescribe for hypogonadism.
In practical terms: a man on prescribed TRT might have a total testosterone of 18 to 25 nmol/L, comfortably within normal range. A man on a typical performance-enhancing steroid cycle might be operating at 60 to 100 nmol/L or above. These are not variations on the same thing. They produce different physiological states.
What medically prescribed TRT actually involves: a blood test to confirm deficiency, clinical assessment, physiological-dose treatment, and ongoing blood monitoring. It is a managed clinical pathway, not a performance intervention.
What TRT is actually treating
TRT is prescribed for male hypogonadism: a clinical condition in which the testes produce insufficient testosterone, producing symptoms that genuinely affect quality of life.
Testosterone declines naturally with age. According to the NIHR TestES evidence synthesis published in 2024, circulating testosterone declines by approximately 1% per year from the age of 40 onwards, and 33 to 50% of middle-aged men have decreased serum levels of the hormone. The subset who have both low levels and clinical symptoms meeting diagnostic criteria is smaller, but it is a real population of men with a diagnosable condition.
The symptoms are real and they are disruptive: persistent fatigue, reduced strength, low mood, reduced sex drive, difficulty concentrating, and body composition changes despite consistent training. A 2025 UK survey from Imperial College London found that 75% of TRT users reported notable improvements in overall quality of life, with 71% reporting improved mental wellbeing and 69% improved self-esteem. For men with genuine testosterone deficiency, TRT produces real clinical benefits.
In a 2025 UK survey of TRT users (Imperial College London, N=250+), 75% reported notable improvements in overall quality of life, 71% improved mental wellbeing, and 69% improved self-esteem and confidence after starting treatment.El-Osta A et al. Translational Andrology and Urology, 2025. N=250+ UK TRT users. pmc.ncbi.nlm.nih.gov/articles/PMC12170005/
The British Society for Sexual Medicine (BSSM) guidelines on testosterone deficiency are the UK clinical reference standard. They define hypogonadism by both biochemical criteria (total testosterone below 12 nmol/L with clinical symptoms) and require a full clinical assessment before prescribing. TRT is not something you can get from a credible UK prescriber just because you want it.
What steroids are actually doing
Anabolic steroid use for performance enhancement is a fundamentally different intervention. The intent is supraphysiological: to push testosterone and related hormones above the natural range deliberately, in order to exceed the muscle-building capacity the body would have at normal hormone levels.
At these doses, the body detects the elevated exogenous testosterone and responds by suppressing its own production via the hypothalamic-pituitary-gonadal (HPG) axis. Gonadotropin-releasing hormone (GnRH) release from the hypothalamus decreases, LH and FSH from the pituitary fall, and the testes reduce or stop natural testosterone production. In some men, particularly after extended heavy use, this suppression becomes difficult or impossible to reverse. The body loses the ability to regulate its own hormonal production.
TRT at physiological doses also suppresses endogenous production because exogenous testosterone still signals through the HPG axis. This is why fertility is a consideration in men on TRT who want to have children: the suppression of LH reduces sperm production. But the suppression at physiological doses is qualitatively different from the suppression that occurs at supraphysiological doses, and the recovery pathway is generally more predictable.
The risk profile: not the same thing
The health risks of prescribed TRT and anabolic steroid use are not equivalent. This is worth stating clearly because the conflation leads people to either overcalibrate the risks of TRT or undercalibrate the risks of steroid use.
TRT: manageable with monitoring
Prescribed TRT is associated with manageable side effects that are monitored and addressed:
- Haematocrit elevation: Testosterone stimulates red blood cell production. Regular monitoring of haematocrit (the proportion of blood that is red blood cells) is part of standard TRT management. Elevated haematocrit increases blood viscosity and clotting risk, so levels above threshold prompt dose adjustment or therapeutic phlebotomy.
- Reduced fertility: Suppressed LH reduces sperm production. Men on TRT who want to preserve fertility can use human chorionic gonadotropin (hCG) alongside treatment to maintain some testicular function.
- Acne and skin changes: Common, manageable.
- Possible PSA changes: PSA is monitored as part of standard TRT follow-up. A 2024 meta-analysis of 28 randomised controlled trials confirmed TRT does not promote prostate cancer development or progression at therapeutic doses.
Anabolic steroid use: categorically different
At supraphysiological doses, the risk profile changes significantly:
- Cardiovascular risk: Supraphysiological testosterone doses are associated with left ventricular hypertrophy, adverse lipid profiles (elevated LDL, reduced HDL), and increased cardiovascular event risk. These are dose-dependent effects not seen at physiological replacement doses.
- Irreversible HPG suppression: As described above, some men who use high-dose steroids for extended periods cannot restore natural testosterone production even after stopping.
- Liver toxicity: Primarily associated with oral 17-alpha alkylated androgens (not injectable testosterone itself), but relevant in the context of the broad range of AAS used.
- Psychiatric effects: High-dose androgen use is associated with mood dysregulation, aggression, and in some cases dependency. These effects are dose-dependent.
- Polypharmacy complexity: Performance-enhancing steroid use often involves multiple compounds simultaneously, with interactions that are not fully characterised and have no clinical oversight managing them.
Training performance and body composition respond to testosterone, but the dose required to produce supraphysiological gains is four to five times higher than what is used in clinical TRT. The health risks are correspondingly different.
The legal position in the UK
Testosterone is a Class C controlled substance in the UK under the Misuse of Drugs Act 1971. It is legal to possess for personal use without a prescription, but illegal to supply, sell, or import without appropriate authorisation. Prescribed TRT from a licensed prescriber is legal. Buying testosterone from unregulated sources, online marketplaces, or gym networks is not.
This distinction matters practically: counterfeit or unverified testosterone from unregulated sources may contain incorrect doses, contaminants, or entirely different compounds. The MHRA has issued warnings about counterfeit injectable testosterone and other anabolic products containing unknown substances. If the compound you are injecting came from a source that cannot verify what is in it, the risk profile is genuinely unknown.
What prescribed TRT looks like in practice
For men who legitimately have testosterone deficiency and want to understand what clinical treatment involves, here is the actual process through a regulated UK provider like Voy.
First, a blood test. Total testosterone and free testosterone are measured, along with other relevant markers. For TRT to be prescribed through Voy’s supervised pathway, total testosterone needs to be below clinical thresholds, accompanied by symptoms. This is not a process where you describe feeling tired and walk out with a prescription.
Once diagnosis is confirmed, treatment is initiated at a physiological dose designed to restore normal range levels, not exceed them. The goal is not to give you the testosterone of a 19-year-old if you are 45. It is to give you the testosterone of a healthy 45-year-old. Regular blood monitoring through treatment checks testosterone levels, haematocrit, PSA, and other relevant markers. Dosing is adjusted based on those results.
Voy offers TRT with regulated prescribing and clinical monitoring for men who are clinically eligible. The pathway is what separates medically supervised treatment from any other approach.
Testosterone declines by approximately 1% per year from the age of 40. Between 33% and 50% of middle-aged men have decreased serum testosterone levels, though only a minority have both low levels and clinical symptoms meeting the diagnostic criteria for hypogonadism.NIHR TestES evidence synthesis. Health Technology Assessment, 2024. journalslibrary.nihr.ac.uk/hta/JRYT3981
Quick answers
Is TRT the same as taking steroids?
No. Both involve testosterone, but at entirely different doses, with entirely different intent and monitoring. TRT uses physiological doses to restore normal testosterone levels in men with a clinical deficiency. Anabolic steroid use involves supraphysiological doses, typically four to five times higher than TRT doses, to push testosterone above normal range for performance enhancement. The physiological effects, the risk profiles, and the medical context are categorically different.
Will TRT make me bigger?
Not in the way performance-enhancing steroid use does. If you have genuine testosterone deficiency, TRT can restore the muscle-building capacity you have lost as a result of low testosterone. You may see improvements in body composition and strength once your levels are corrected, particularly if you are training. What TRT will not do is produce the supraphysiological muscle gain that comes from doses four to five times higher than replacement level. It is a treatment for a deficiency, not a physique drug.
What are the signs of low testosterone?
Persistent fatigue that is not explained by poor sleep or overtraining, reduced strength and muscle mass despite consistent training, low mood or reduced motivation, reduced libido, difficulty concentrating, and increased body fat particularly around the abdomen. These symptoms overlap with a lot of other conditions, which is why a blood test is required to confirm diagnosis. Symptoms alone do not confirm testosterone deficiency.
Is TRT legal in the UK?
Prescribed TRT is legal. Testosterone is a Class C controlled substance in the UK. Possession for personal use is not an offence, but supply and sale without authorisation are. A valid prescription from a registered UK prescriber makes TRT legal to obtain and use. Purchasing testosterone from unregulated sources, including online marketplaces or through gym networks, does not have the same legal protection and carries additional safety risks from unknown product quality.
How does TRT affect training?
For men with genuine testosterone deficiency, restoring normal testosterone levels can meaningfully improve training performance. Low testosterone is associated with reduced muscle protein synthesis, slower recovery, reduced motivation, and lower energy. Correcting the deficiency restores your baseline capacity. You will not have an unfair advantage in the gym because of TRT. You will have the hormonal baseline that men without deficiency already have.
What monitoring does TRT involve?
Standard TRT monitoring includes regular blood tests checking total testosterone (to confirm levels are in the therapeutic range), haematocrit (to monitor red blood cell production and blood viscosity), PSA (prostate-specific antigen, as part of prostate health monitoring), and liver function. The frequency varies by provider and how stable your levels are, but ongoing monitoring is a non-negotiable component of safe TRT. If a prescriber does not require ongoing blood tests, that is a significant warning sign.
| This article is for informational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before starting any hormone treatment. Individual results may vary. Treatment is subject to clinical suitability assessment. |
Sources
• Voy. Is testosterone a steroid? joinvoy.com/blog/is-testosterone-a-steroid
• El-Osta A et al. A cross-sectional survey of experiences and outcomes of using testosterone replacement therapy in UK men. Translational Andrology and Urology, 2025. N=250+. pmc.ncbi.nlm.nih.gov/articles/PMC12170005/
• Cruickshank M, Hudson J et al. The effects and safety of testosterone replacement therapy for men with hypogonadism: the TestES evidence synthesis. NIHR Health Technology Assessment, 2024. journalslibrary.nihr.ac.uk/hta/JRYT3981
• British Society for Sexual Medicine (BSSM). Guidelines on adult testosterone deficiency. bssm.org.uk/resources/guidelines/
• Bhasin S et al. The effects of supraphysiologic doses of testosterone on muscle size and strength in normal men. New England Journal of Medicine, 1996.
• MHRA. Counterfeit and unlicensed testosterone product warnings. GOV.UK.